6. Curating model parameters
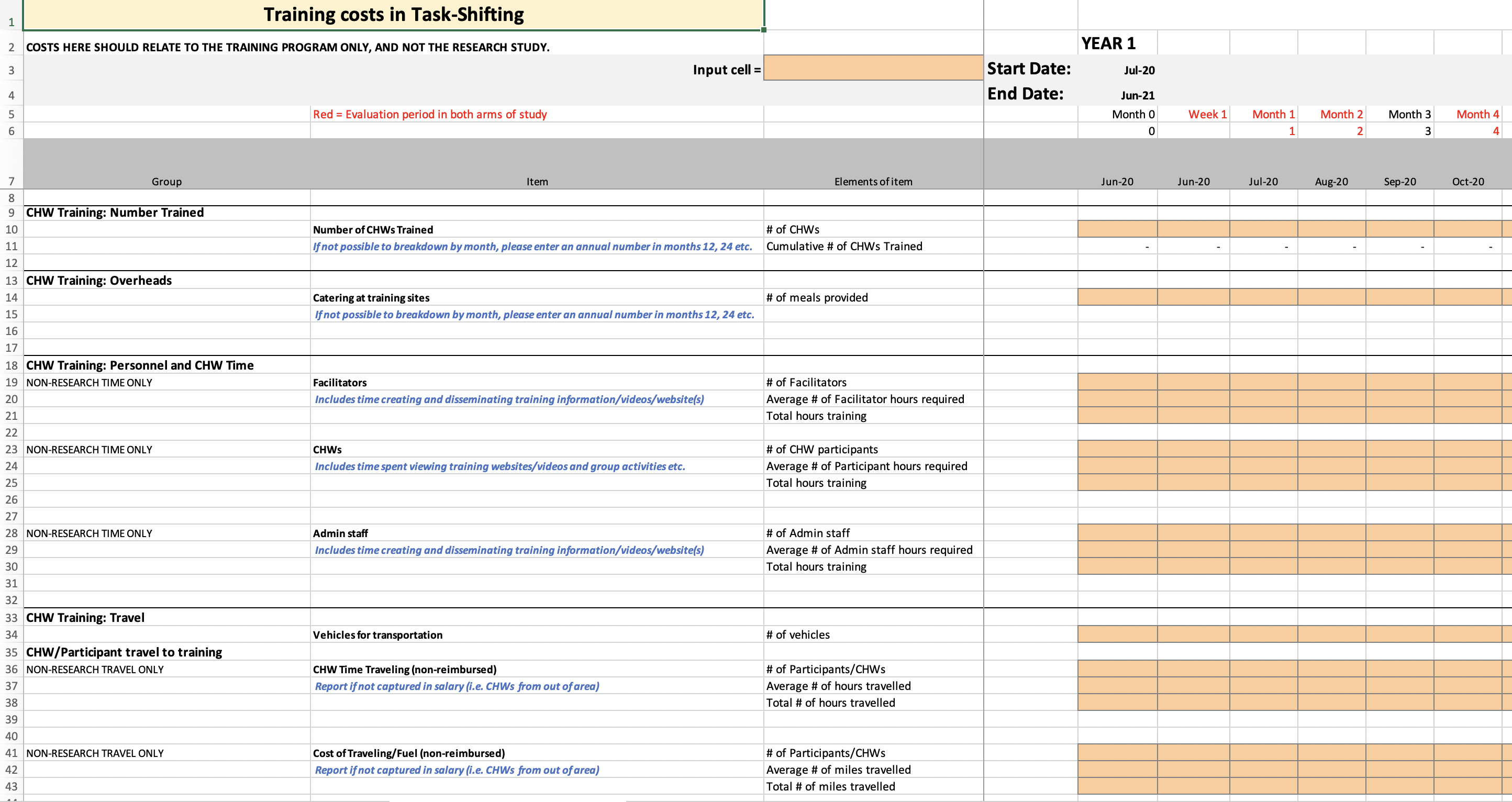
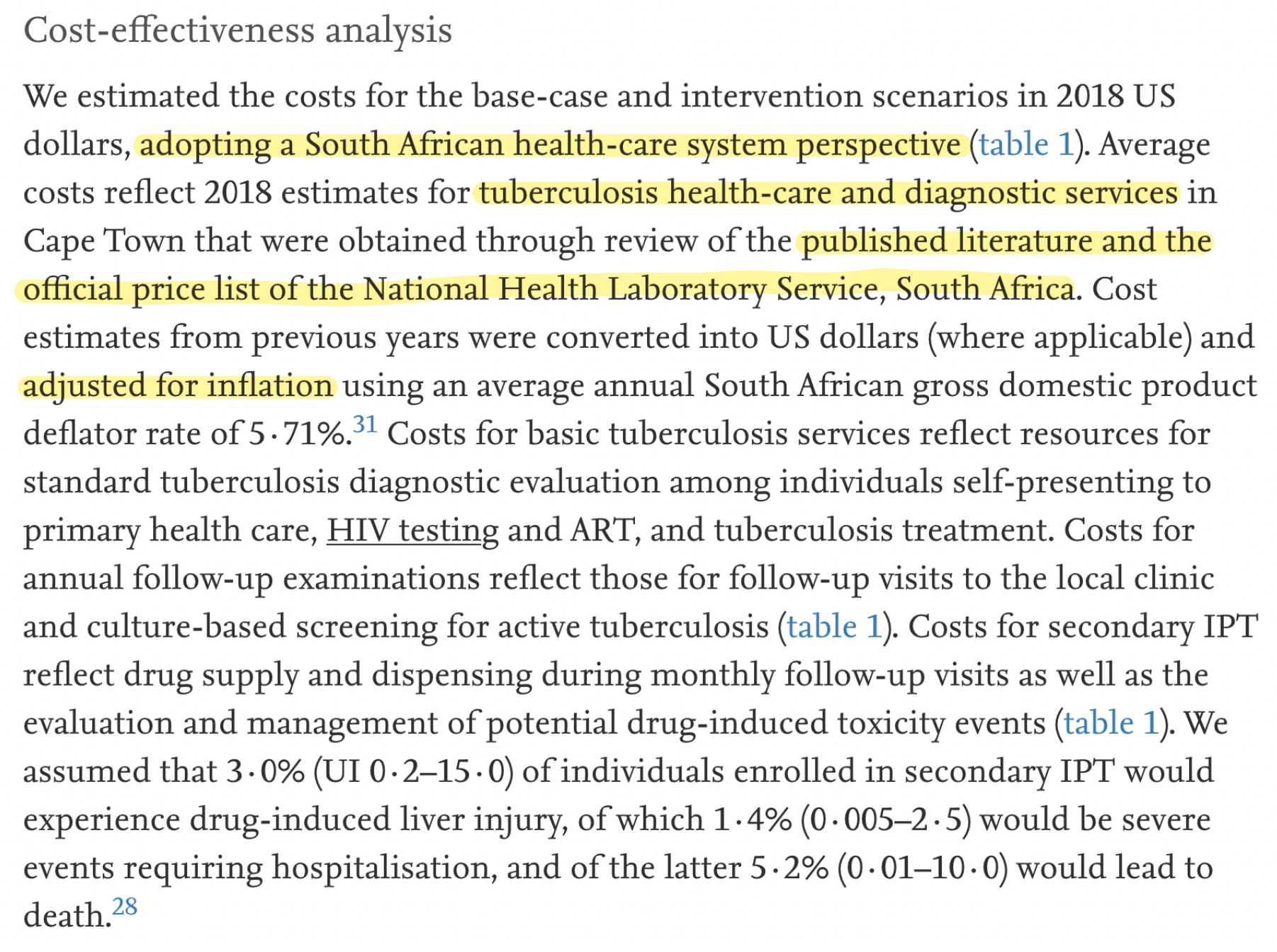
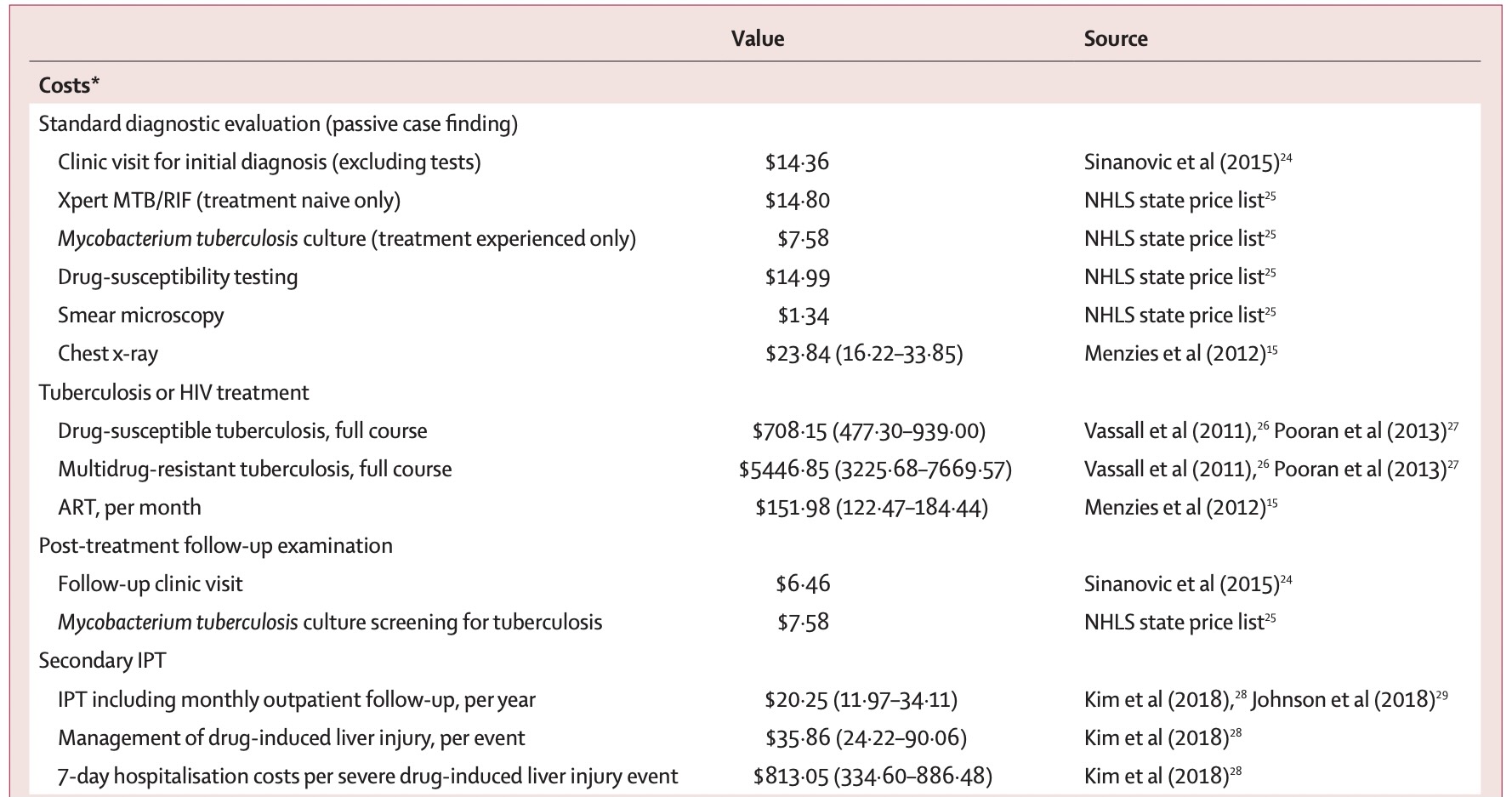
Costs (clinical trials)
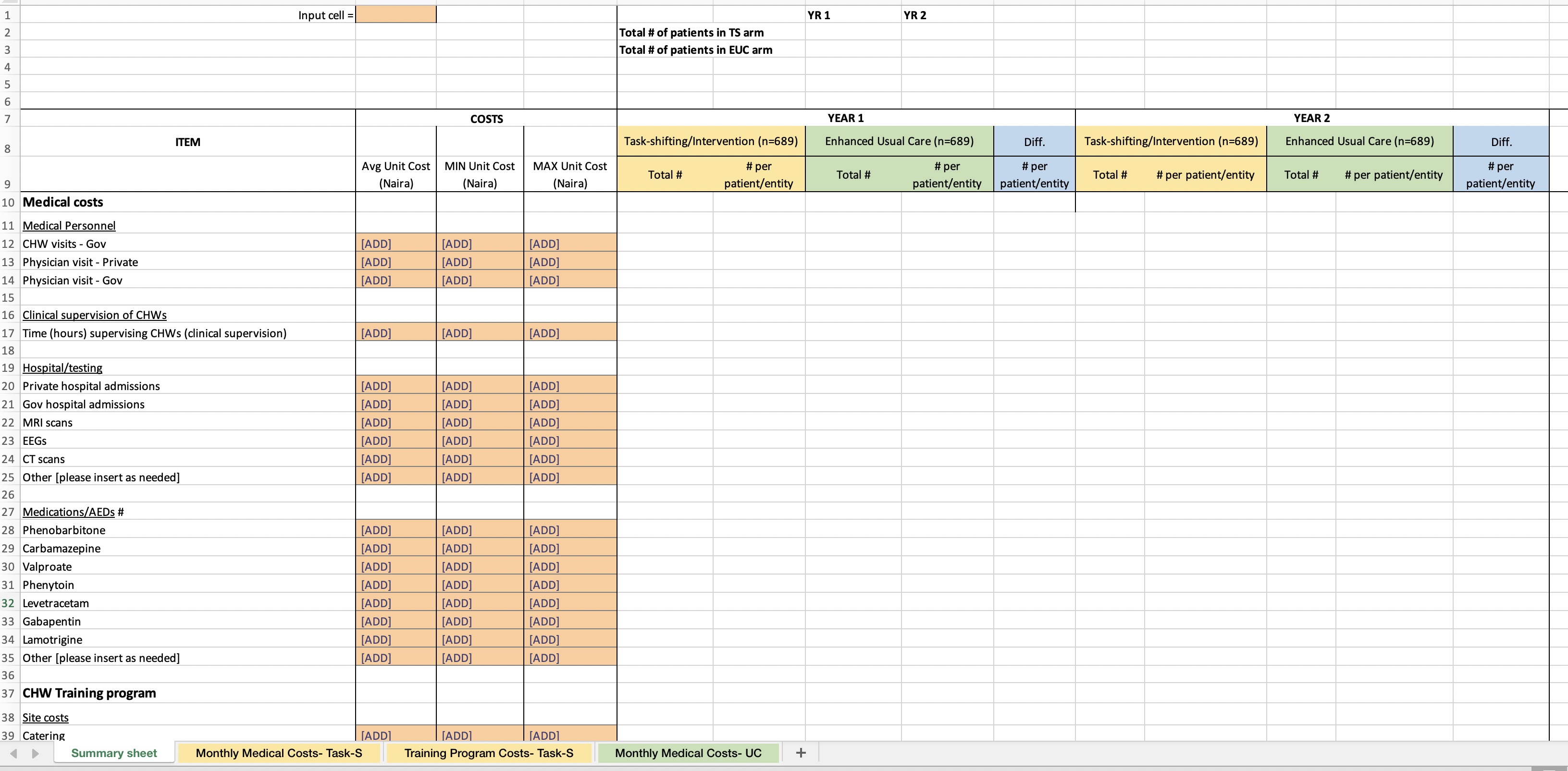
Costs (clinical trials)

Costs (clinical trials)
Costs (secondary data)
Costs (secondary data)
Costs (secondary data)
Costs (secondary data)
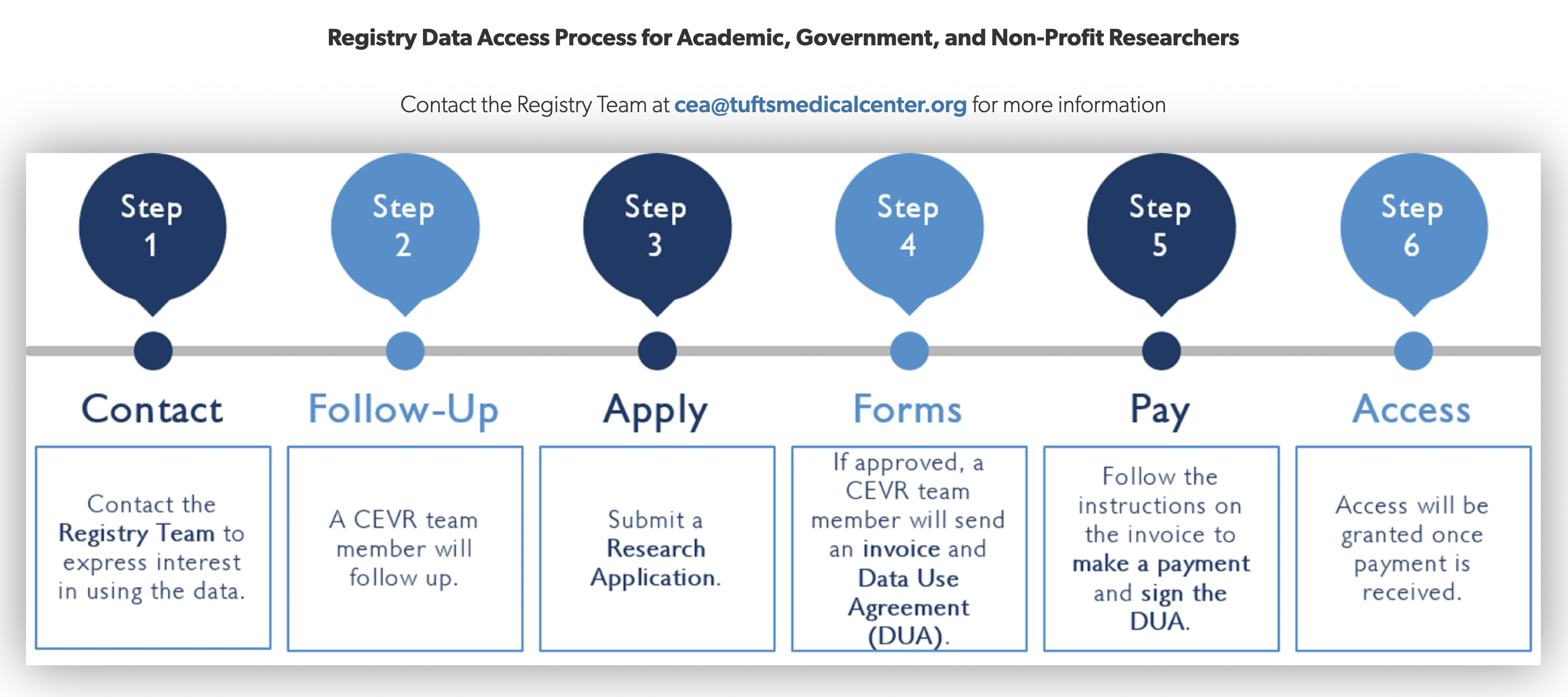
https://cevr.tuftsmedicalcenter.org/databases/cea-registry
Costs (secondary data)

Costs (secondary data)
Costs (secondary data)
Costs (secondary data)
Costs (secondary data)

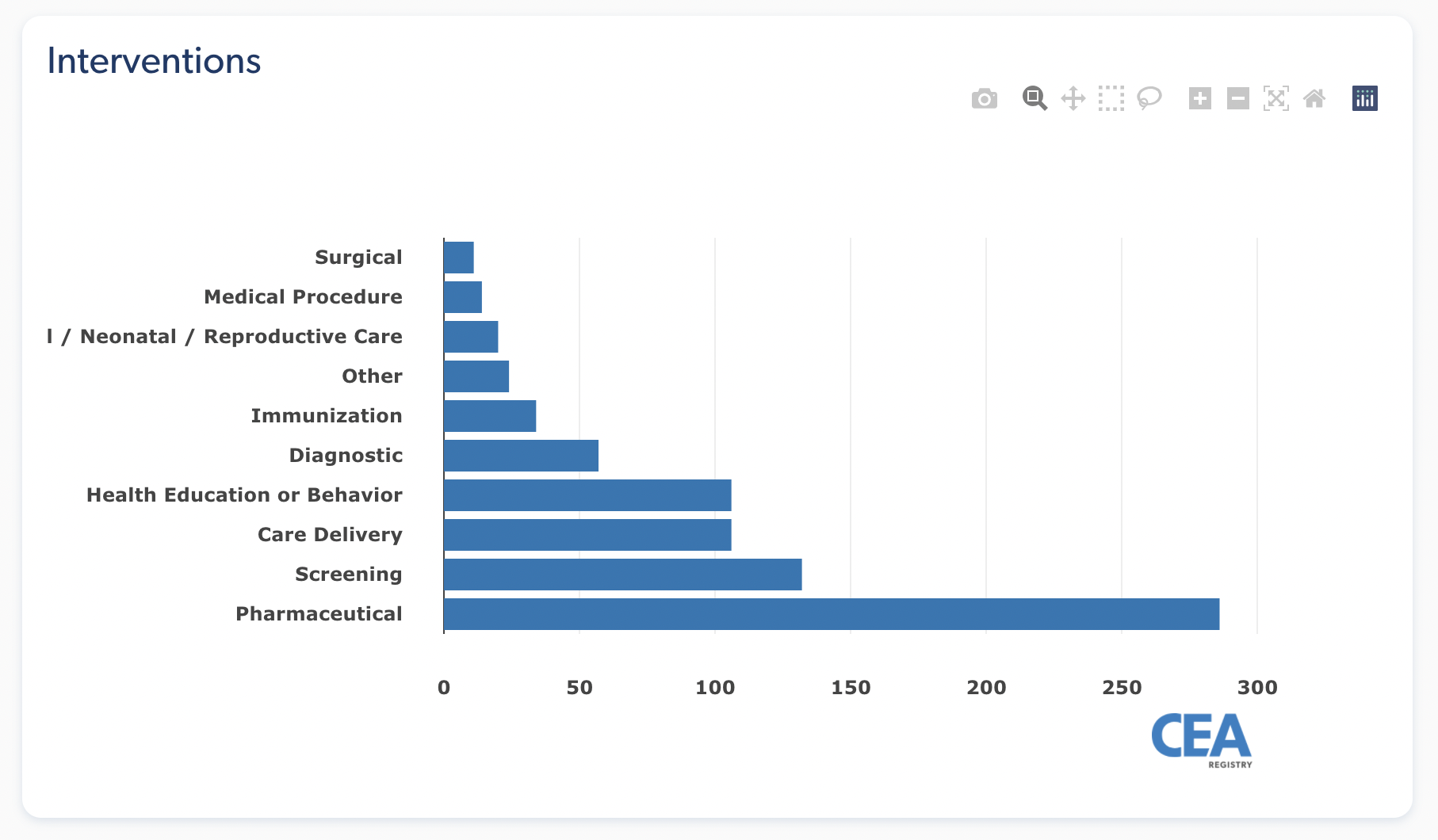
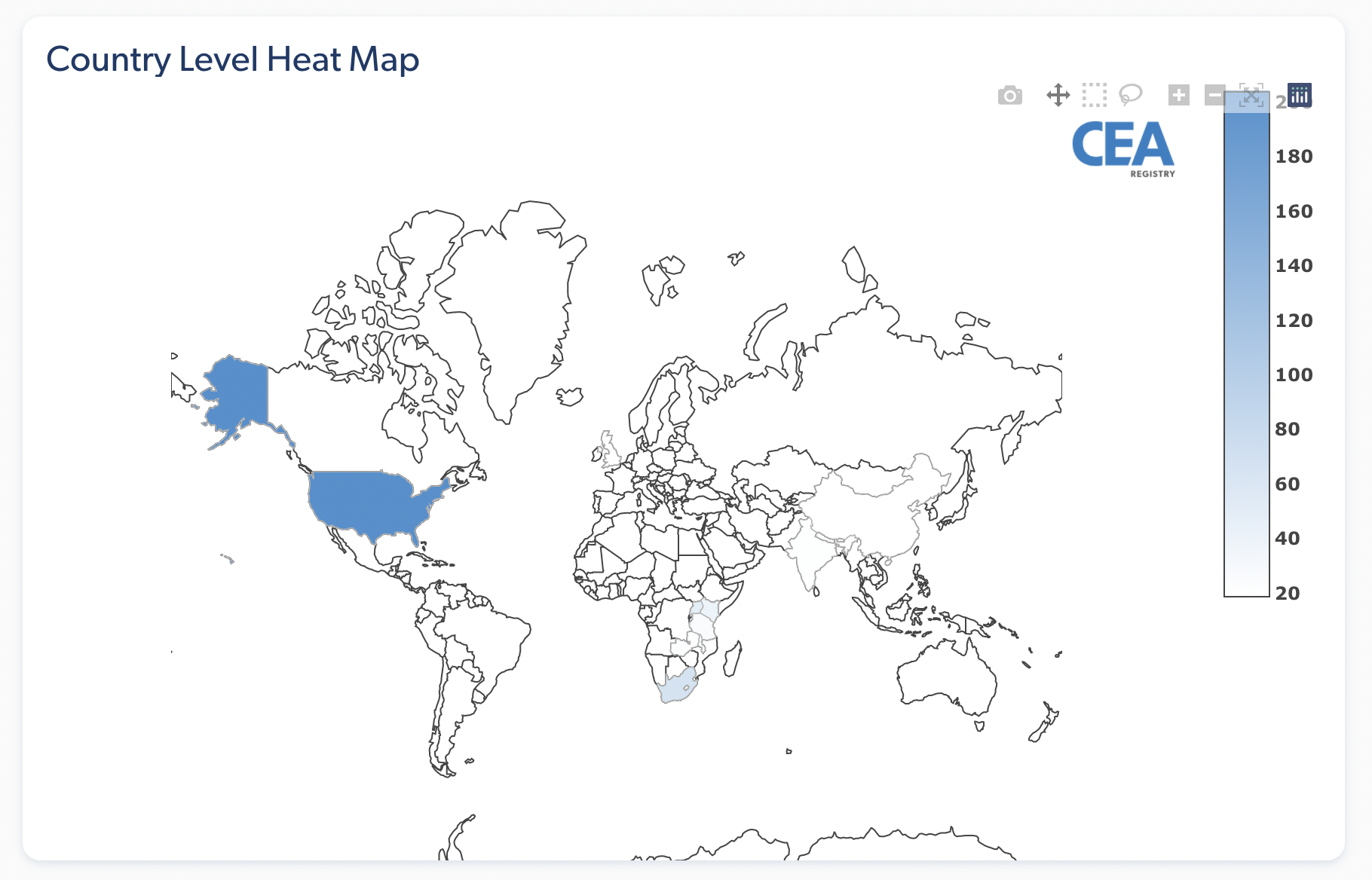
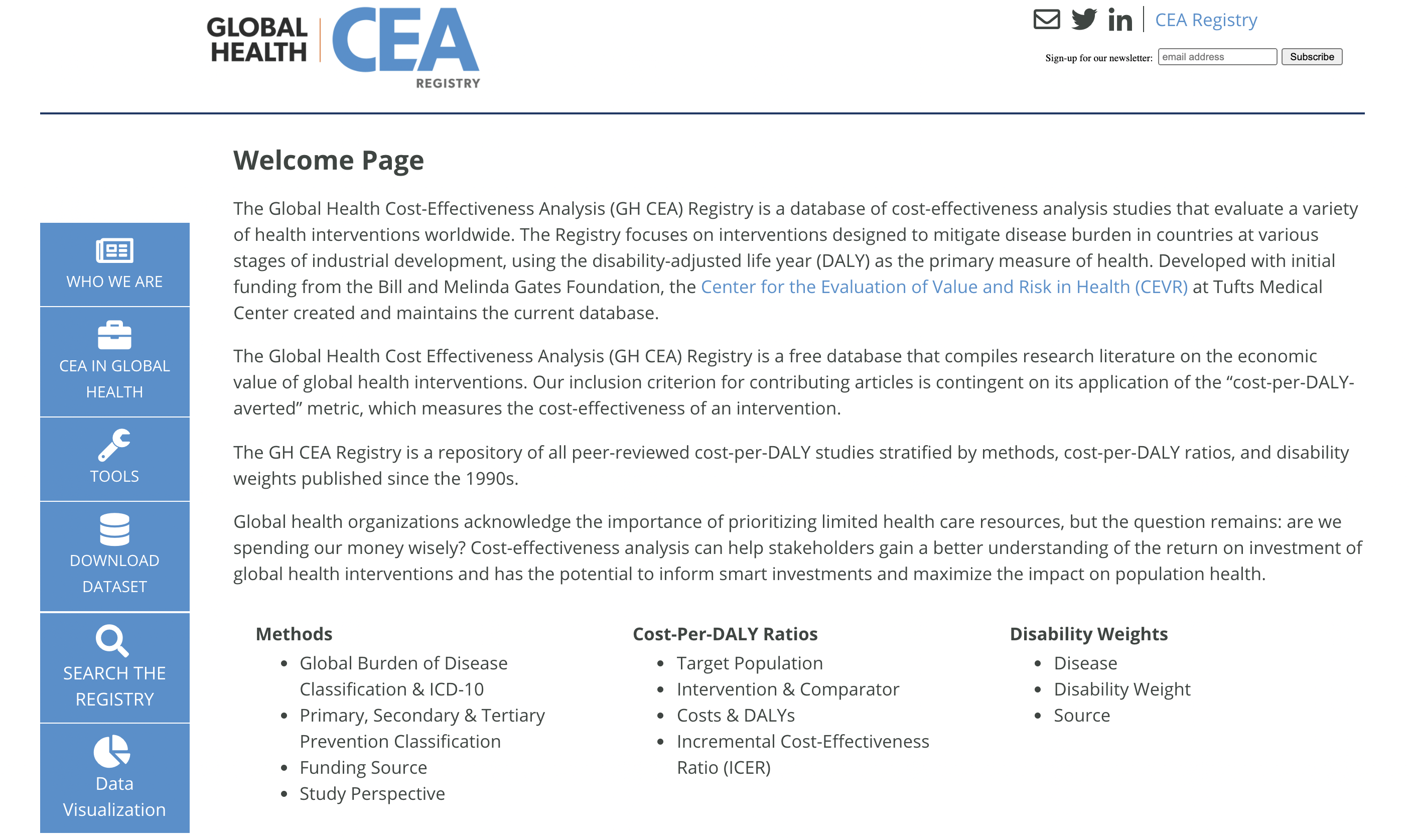
http://ghcearegistry.org/ghcearegistry/
Costs (secondary data)
Costs (secondary data)
Costs (secondary data)

Costs (secondary data)
Costs (secondary data)

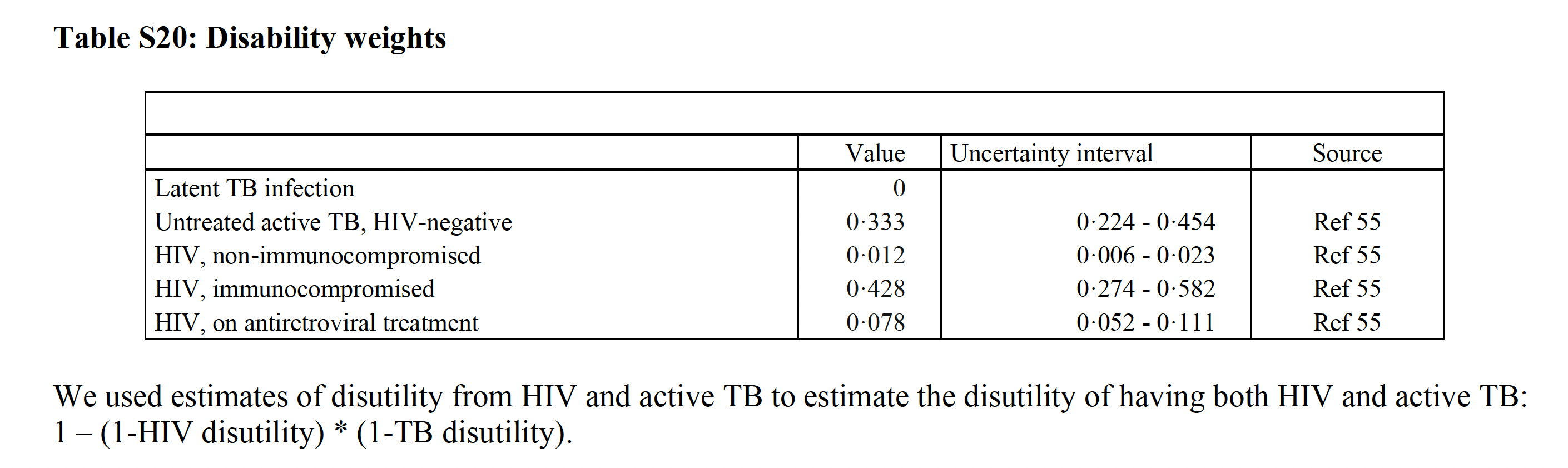
Effects (secondary data)
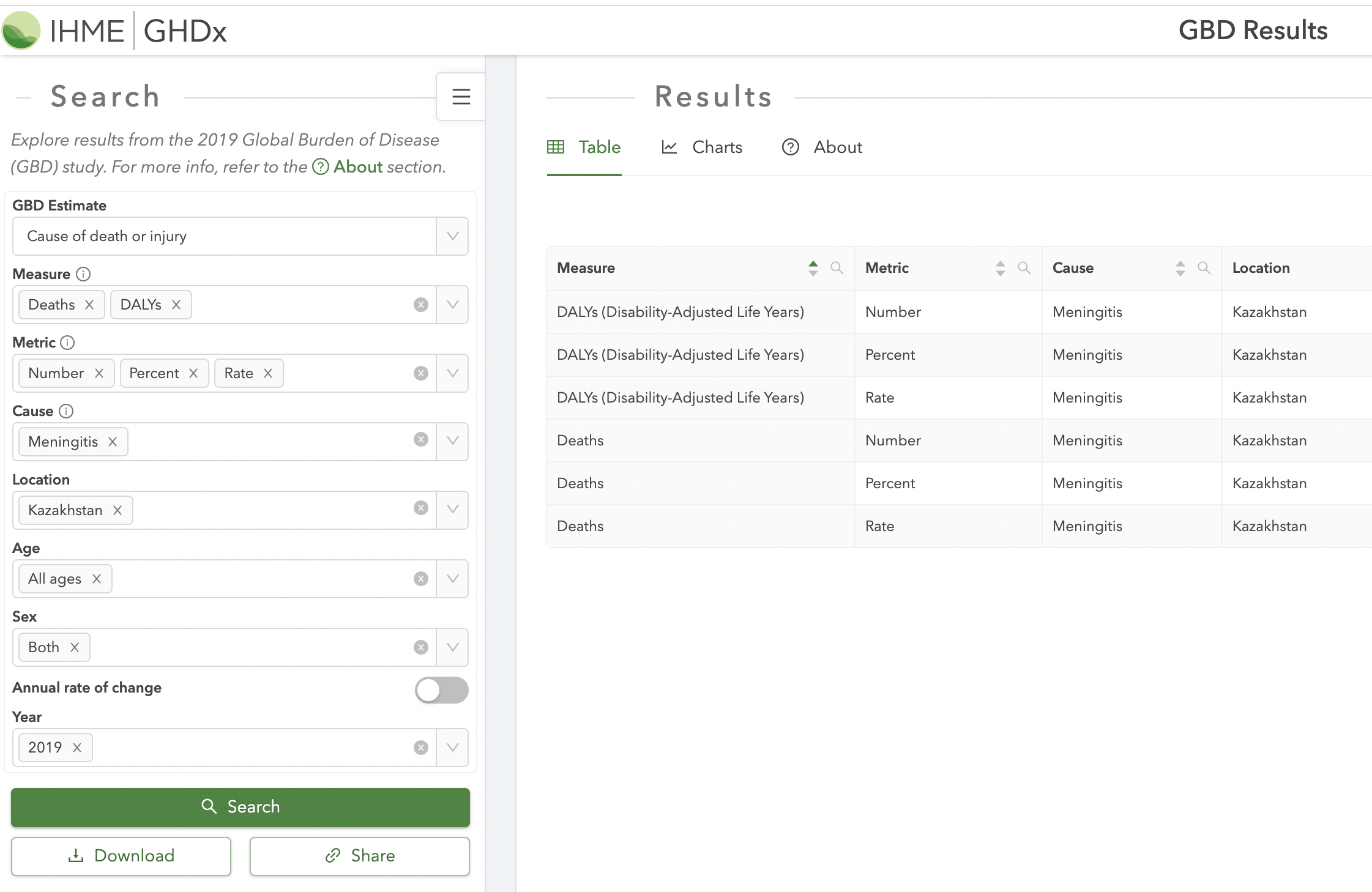
Effects (secondary data)
(Marx et al 2020)
Effects (secondary data)
(Marx et al 2020)
Effects (secondary data)

Effects (secondary data)

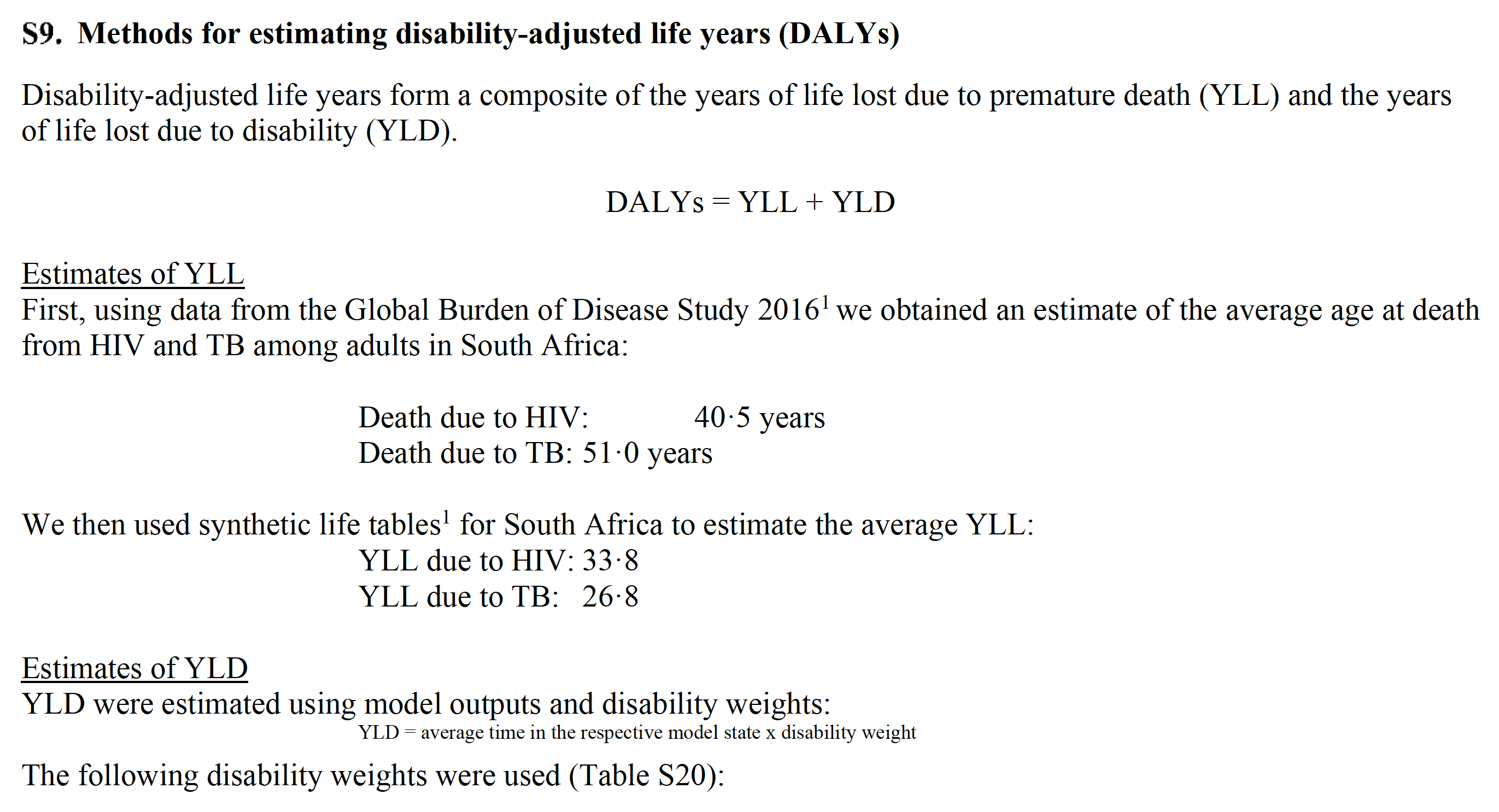
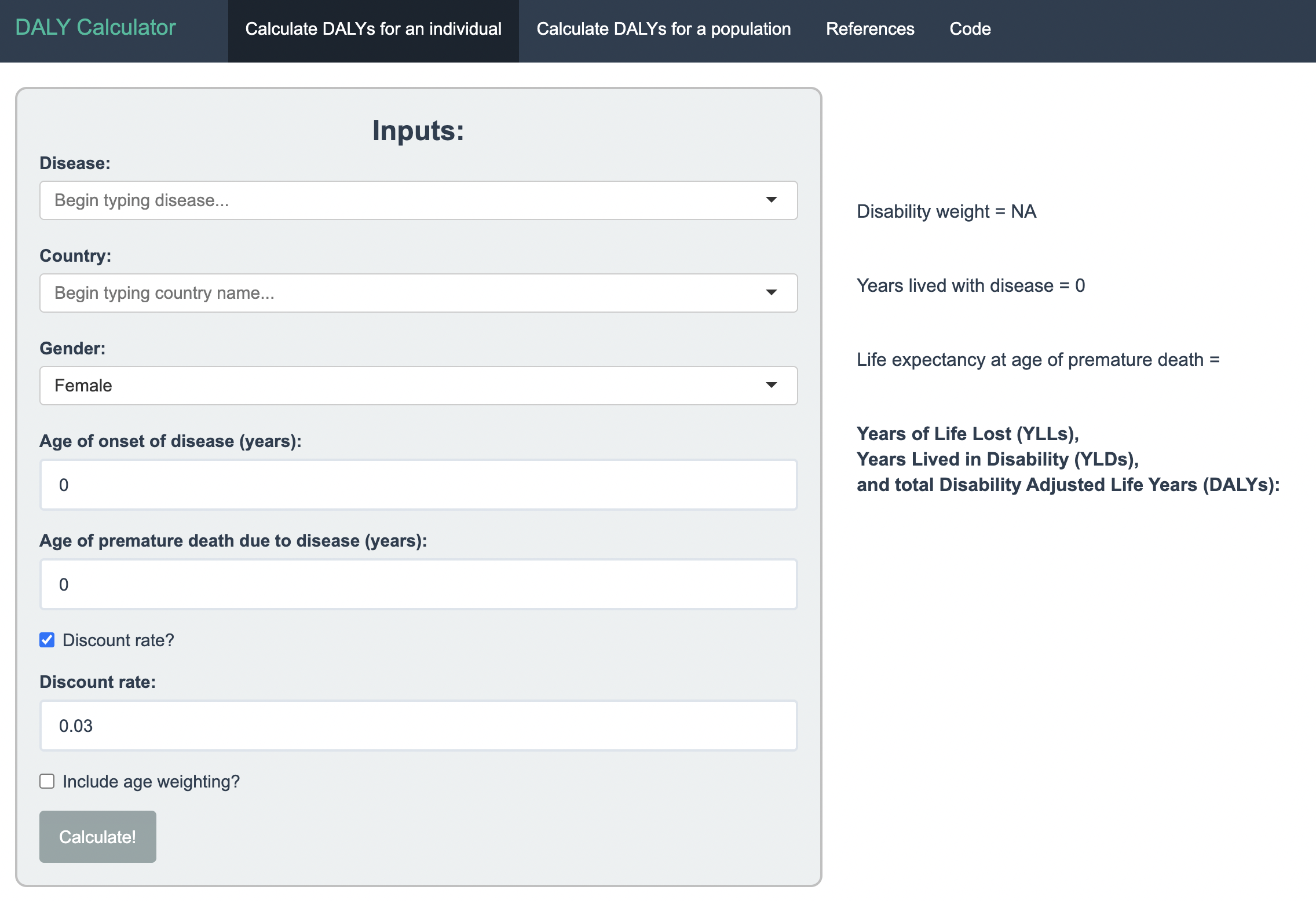
A tool that can convert health outcomes expressed in non-DALY metrics (e.g., cases or deaths averted) into DALYs – converted DALY measures can then be used to compare cost-effectiveness ratios of interventions across different disease areas (http://ghcearegistry.org/ghcearegistry/)
Effects (secondary data)
Effects (secondary data)